Coronary heart disease occurs when there is a decrease in blood supply to the heart muscles due to narrowing and obstruction of the coronary arteries. This leads to myocardial ischemia, the lack of oxygen to the heart. Furthermore, it leads to a high demand for o2 due to myocardial hypertrophy due to hypertension.
This can be produced by thrombosis, where adhesion of platelets at plaque occur or plaque rupture occurs. Anaemia and hypertension are also the causes of this.
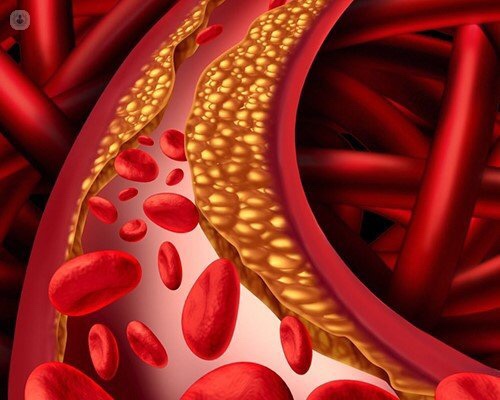
However, the main cause of coronary heart disease is atherosclerosis, where accumulation of lipids, macrophages and smooth muscle create a plaque. This dysfunction/ injury of the endothelium is caused by several factors such as mechanical stress (e.g. hypertension), biochemical abnormalities (e.g. diabetes, elevated LDL levels), genetics, infection and free radicals.
This injury increases the accumulation and permeability of oxidised LDL’s, which in turn is taken up by macrophages to generate foam cells causing fatty streaks.
This will progress further into a transitional plaque with the addition of extracellular lipids. Cholesterol precipitates into crystals, causing cell necrosis.
Cytokines are released by macrophages. Furthermore, the endothelium damage recruits more macrophages and promotes smooth muscle cell proliferation.
Collagen is produced by the smooth muscle cells leading to secondary fibrosis.
Cholesterol crystals, enzymes and debris leak out to induce calcification. This will lead to irreversible degenerate changes leading to a stable plaque.
Clinical manifestations are variable, where they can be asymptomatic (free of symptoms), cause angina pectoris or if severe and prolonged, can cause a heart attack.
Symptoms can include: Dizziness, fatigue, shortness of breath and chest discomfort.

