The roles of clinical microbiologists include the identify- cation of bacterial, viral, fungal and parasitic agents that cause human disease, providing diagnostic and therapeutic support for the clinical management of patients, and preventing the transmission of infectious diseases in both the health care system and the community.Developments in sampling: he conventional diagnosis of infectious diseases usually relies on a step- wise approach in which the physician examines the patient, diagnoses a clinical syndrome and then tests for pathogens that are potentially responsible for that syndrome, until a diagnosis is made. However, the growing number of emerging pathogens makes it difficult for physicians to memorize the actual list of pathogens for each infectious disease and thus prescribe all the appropriate diagnostic microbiology tests.
Identification and resistance testing ofpathogens:
Identification of bacteria, fungi and viruses.Phenotypic identification of bacterial isolates has long relied on a combination of biochemical properties such as oxygen requirement, Gram staining, carbohydrate metabolism and the presence of specific enzymes. However,phenotypic identification systems, such as miniaturized strips, are costly and time-consuming.
Direct microbial identification in specimens:
Mass spectrometry.In 2009, for the first time, MALDI–TOF MS was reported to efficiently identify bacteria directly from blood collected in culture bottles, with results obtained less than 2 hours after the blood culture vial was determined to bepositive, and with a 97.5% success rate. However, the accuracy of bacterial identification might be influenced by unstandardized sample preparation, differences in bacterial concentrations, pre-incubation, prolonged incubation and the blood culture system used.
Sequencing of microbial genomes:
Genomic sequence information from cultivated micro- organisms is widely used for epidemiological studies (TABLE 1). In clinical microbiology, applications of genome sequencing include the development of detection, identification and genotyping tools, the design of culture media and the assessment of antibiotic resistance or virulence repertoires
With the introduction of omics technologies (genomics, proteomics, culturomics, transcriptomics and metabolomics), CMLs face new challenges, such as obtaining a diagnosis at the time of care (FIG. 4). For example, until recently, the usefulnessof blood cultures in the emergency room was limited, as the results of identification and antibiotic-susceptibility testing were only available 72 hours after sampling. Under these conditions, either the empirically prescribedantibiotic treatment was effective, or it had to be changed to another treatment, the worst-case scenario being the patient’s death before the diagnosis was established. Clearly, CMLs can only have a major impact on early patient management when diagnostic speed enables the appropriate medical decisions to be made rapidly. In terms of treatment, rapid pathogen identification combined with knowledge about where the patient contracted the infection (for example, whether it was hospital acquired or community acquired) enables the presumptive deduction of antimicrobial susceptibility, and such antibiotic stewardship based on rapid diagnostics can reduce hospitalization costs.
The alternatives to classsic antibiotics include using traditional methods, exploiting natural resources and the use of bacteriophages.
Honey, plant and invertebrate extracts:
Honey is known for its antimicrobial properties – these include low pH, hydrogen peroxide production (in some honeys), high osmolarity, flavonoids and likely undiscovered antimicrobial compounds. The ‘quality’ of the honey varies with what it is grown on – so the plants make a difference. Honey can used as a wound dressing (topical application), but other applications are trickier due to dilution. Plant extracts have been used in traditional medicine for millennia and have largely been forgotten in the west as some believe antibiotics provided a ‘better’ treatment. Research on antimicrobial phytochemicals is dominated by articles coming from China, the Indian subcontinent and Saudi Arabia. Thousands of compounds have been listed as possessing antimicrobial properties.
However, cost-effective methods of extraction and purification of phytochemicals is a major concern as well as safety and translatability. In addition, a big part of plant and invertebrate resistance are their innate immunity and antimicrobial peptides. Invertebrates and plants have innate immunity pathogen-associated molecular pattern (PAMP)-recognising proteins and respond to infection by synthesis of antimicrobial peptides (AMPs). Overall, about 1200 structures have been described in animals, microbes and plants. The peptides are often short and have no conserved sequence.
Teixobactin:
Teixobactin is an oligopeptide antibiotic produced by a Gram-negative bacterium, Eleftheria terrae. Teixobactin is bacteriocidal, has a stable and potent activity against S. aureus and at least over a short-term experiment, shows no induction of resistance in vitro. Teixobactin attacks both peptidoglycan as well as teichioinic acid production. By attacking two pathways, resistance is much harder to achieve.
Despite the advantages, the problem with this approach is that screening tens of thousands of possibilities is expensive, and people have tried it before – in fact more antibiotics are known than are used. Other options do not work well enough or toxic or both.
Bacteriophages:
Bacteriophages are viruses that infect bacteria. There are 10 times more bacteriophages than there are bacteria. Bacteriophages infect and lyse the bacterial cell like most other viruses.
Advantages and Disadvantages:
They have many advantages over antibiotics including:
o Lower emergence of resistance if ‘cocktails’ are used.
o High host specificity, sometimes to species or even strain level.
o Limiting pleiotropic effects on gut microflora and other negative effect on the human host – Bacteriophage can have a lytic and a lysogenic cycle, making temperature (fever)-induced lysis of the bacterial pathogen possible.
o Advances in sequencing have led to massive discoveries.
There are disadvantages:
o Not all phages lyse their host
o High host specificity renders the phages useless against unknown pathogens
o There are, for example, 2,500 Salmonella enterica serovars, only few of which have known lytic phages.
o Bacteriophage can temporarily integrate into the host genome prior to lysis leading the possibility of horizontal gene transfer.
o Phages are foreign particle leading to antibody production.
o Not yet licenced for systemic therapy in humans.
Thedifferent types of skin infectionsinclude bacterial, viral and fungal.
Symptoms within this can vary from mild to serious. Mild infections may be treatable with over-the-counter medications and homeremedies, whereas other infections may require medical attention.
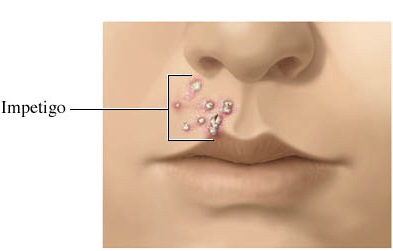
Impetigois a skin infection caused by bacteria. It is usually caused by either groupAβ-hemolyticstreptococciorStaphylococcusaureus.
It is most common in children between the ages of two and six. It usually starts when bacteria get into a break in the skin, such as a cut, scratch, or insect bite. Impetigo is a skin infection caused by bacteria. It is most common in children between the ages of two and six.
It usually starts when bacteria get into a break in the skin, such as a cut, scratch, or insect bite. Other symptoms includefluid-filled blisters,itchy rash,skin lesionsandswollen lymph nodes.Impetigo can spread by contact with sores or nasal discharge from an infected person, other causesinclude contactwith sores or nasal discharge from an infected person.youcan treat impetigo with antibiotics.toxinsare the greatest virulence factor ofS.aureus, causing dissociation of epidermal cells with blister formation. Crucial factor to the infection virulence is the ability of these bacteria to produce circulating toxins that act assuperantigens.Superantigensare able to skip certain steps of the immune response and promote massive activation of T lymphocytes and also the production of variouslymphokinessuch as interleukin 1 and 6 andtumornecrosis factor alpha. This response may lead to the formation ofexfoliativecutaneous eruption, vomiting, hypotension and shock.
Shinglesis a disease caused by the varicella-zoster virus – the same virus that causes chickenpox.
After you have chickenpox, the virus stays in your body. It may not cause problems for many years. As you get older, the virus may reappear as shingles. Although it is most common in people over age 50, anyone who has had chickenpox is at risk.
You can’t catch shingles from someone who has it. However, if you have a shingles rash, you can pass the virus to someone who has never had chickenpox. This would usually be a child, who could get chickenpox instead of shingles. The virus spreads through direct contact with the rash, and cannot spread through theair.Earlysigns of shingles include burning or shooting pain and tingling or itching, usually on one side of the body or face. The pain can be mild to severe. Rashes or blisters appear anywhere from one to 14 days later. If shingles appears on your face, it may affect your vision or hearing. There is no cure for shingles. Early treatment with medicines that fight the virus may help. These medicines may also help prevent lingering pain.A vaccine may prevent shingles or lessen its effects.Oneof thevirualncefactors for thisviral infection is adhesion of the virus to specific receptors on the surface of cells. This process is mediated byadhesinsthat are part of the viral capsid or membrane envelope. The interaction of viraladhesinswith specific cell receptors defines the tropism(preferential targeting) of viruses for specific cells, tissues, and organs in the body. The spike protein hemagglutinin found onInfluenzavirusis an example of a viraladhesin; it allows the virus to bind to thesialicacid on the membrane of host respiratory and intestinal cells.
Athlete’s foot — also calledtineapedis— is a contagious fungal infection that affects the skin on the feet and can spread to the toenails and sometimes the hands. Athlete’s foot occurs when thetineafungus grows on the feet. You can catch the fungus through direct contact with an infected person or by touching surfaces contaminated with the fungus. The fungus thrives in warm, moist environments and is commonly found in showers, on locker room floors, and around swimming pools.Symptoms include,itching, stinging, and burningbetween thetoes,itching, stinging, and burning on the soles of the feetandblisters on the feet that itch.Athlete’s foot can often be treated with over-the-counter (OTC) topical antifungal medications. Virulencefactors include the active abstraction ofsome nutrients from host molecules, for example, nitrogen from host proteins by secreted proteaseactivities. Fungal infection also led to theacquisition of micronutrients such as metals, since the host has evolved mechanisms to deny access to metals like zinc or iron (known as ‘nutritional immunity’).In turn, fungal pathogens have developed sophisticated strategies to gain iron, zinc and other metals from the host. Similarly, to survive in the host fungal pathogens must exhibit physical robustness (e.g. conferred by a protective cell wall)and stress resistance (e.g. against reactive oxygen species (ROS) or must be able to manipulate environmental conditions like the ambientpH.
A drug is any chemical taken that has the ability to affect the way the body works; examples include aspirin and nicotine. New drugs are needed as a great deal of medical needs remain unmet. These needs include the emergence of new diseases, the low efficacy of existing drugs and the use of drugs that have too many side effects. Pharmaceutical companies tend to concentrate on developing drugs for diseases which are prevalent in developed countries e.g. cancer and cardiovascular diseases and aim to produce compounds with better properties than existing drugs.
Drug discovery phase
Pre-discovery, researchers gather as much information as possible about the disease and try to understand its nature. The next step is target identification; researchers choose a molecule in the body to target with a drug; often a protein molecule e.g. an enzyme. The chosen target is then tested to confirm its role in the disease. A ‘lead compound’ is then found; this is a molecule that has the potential to become a drug. Early safety tests are then conducted on the lead compound; the pharmacodynamics and pharmacokinetics of the drug are then determined. Pharmacodynamics explores what a drug does to the body, whereas pharmacokinetics explores what the body does to the drug. The next step is to check the drugs ADMET (Absorption, Distribution, Metabolism, Excretion and Toxicity) properties. The final step of the drug discovery phase is lead optimization. The chemical structure of the lead compound is used as a starting point for chemical modifications in order to improve potency, selectivity, or pharmacokinetic parameters.
The development phase
The first stage is pre-clinical testing, in vitro and in vivo tests are carried out to determine whether the drug is safe enough for human testing. A clinical trial exceptions (CTX) application must then be filed with appropriate authorities before clinical testing can begin. During phase 1 clinical trials, the drug is tested on a small group of healthy volunteers to determine toxicity relative to dose and to screen for unexpected side effects. Phase 2 clinical trials consist of the drug being tested on a small group of patients to see if it has any beneficial effect and to determine the dose level needed for this effect. During phase 3 clinical trials, the drug is tested on a much larger group of patients and the results are compared with existing treatments as well as a placebo to show its efficacy. Drug developers then apply to the appropriate authorities (FDA) for approval; if approved, full-scale production of the drug begins. Phase 4 trials consist of continuous monitoring of the drug in use. The drug is placed on the market and patients are monitored for side effects.
The current treatments for many autoimmune diseases include the systemic use of anti-inflammatory drugs and potent immunosuppressive and immunomodulatory agents (i.e., steroids and inhibitor proteins that block the action of inflammatory cytokines). In recent years, researchers have contemplated the use of stem cells to treat autoimmune disorders such as Lupus, Rheumatoid arthritis and Type 1 diabetes.
Gene therapy is the genetic modification of cells to produce a therapeutic effect. In most investigational protocols, DNA containing the therapeutic gene is transferred into cultured cells, and these cells are subsequently administered to the animal or patient. DNA can also be injected directly, entering cells at the site of the injection or in the circulation. Under ideal conditions, cells take up the DNA and produce the therapeutic protein encoded by the gene. There are several approaches for isolating and cultivating stem cells or islet precursor cells from fetal and adult pancreatic tissue. In addition, new promising studies indicate that insulin-producing cells can be cultivated from embryonic stem cell lines.
Development of Cell-Based Therapies for Diabetes
Mouse embryonic stem cells can be derived from the inner cell mass of the early embryo (blastocyst) and cultured under specific conditions. The embryonic stem cells can then be expanded and differentiated. Islet cells can be selected for further differentiation and characterisation. These cells can then be grown in culture where they spontaneously form three-dimensional clusters similar in structure to normal pancreatic islets. The cells also produce and secrete insulin. The pancreatic islet-like cells show an increase in release of insulin as the glucose concentration of the culture media is increased. The pancreatic islet-like cells became vascularized, synthesized insulin and maintained physical characteristic when implanted in the shoulder of diabetic mice.
Stem Cells Bring New Strategies for Developing Replacement Neurons
Furthermore, this same method of using mouse embryonic stem cells from the inner cell mass of the blastocyst and culturing these cells until the create embryoid bodies. The embryoid cells are differentiated. Nestin-positive neuronal precursor cells or Islet cells can be selected for further differentiation and characterisation. These cells can produce dopamine or serotonin and can be used as neurotransmitters that cross synapses and bind receptors on the neuronal cell body and dendrites. This can be a potential therapeutic treatment for Parkinson’s disease were the nigro-striatal pathway degenerates for unknown reasons.
Stem Cells’ Future Role in Spinal Cord Injury Repair
Researchers used a rat model of amyotrophic lateral sclerosis (ALS) which is a disease that destroys special nerves found in the spinal cord, known as motor neurons, that control movement. Using stem cells from fetal tissue which were cultivated under certain conditions to produce embryoid bodies that look and function like neurons. Only elected cells that displayed molecule markers of neural stem cells, including the proteins nestin and neuron specific enolase were selected for further differentiation. The prepared cells from embryoid bodies were injected into fluid surrounding the spinal cord of the paralysed rats that had damaged motor neurons. The results showed that the rats had regained motor abilities. This shows potential therapeutic treatment for patients of Motor Neuron diseases, Multiple Sclerosis, Alzheimer’s disease and Huntington disease where the nerves are damaged.
Nosocomial infections are contracted because of an infection or toxin that exists in a certain location, such as a hospital. People now use nosocomial infections interchangeably with the terms health-care associated infections (HAIs) and hospital-acquired infections. HAI infections can occur, 48 hours after hospital admission, 3 days after discharge and 30 days after an operation. Examples of nosocomial infections include staphylococcus aureus, pseudomonas, aeruginosa, Surgical site infections, meningitis, urinary tract infections (UTIs).
Any patient is at risk for developing an HAI, although there are certain factors that increase the risk of infection. These include, for example, patient characteristics, such as, age or underlying diseases or conditions that may compromise the immune system; presence of indwelling or invasive medical devices, such as catheters or breathing tubes; complications from surgical procedures; and antibiotic use. The risk of infection related to invasive devices increases the longer the device is left in place. Patients in the healthcare setting are also at increased risk of HAIs from exposure to organisms that are transmitted between patients and healthcare workers.
There appears to be a direct relationship between increasing age and susceptibility to infections this means that elderly people are more likely to have nosocomial infections. Other vulnerable people include, pregnant woman, very young children such as premature babies and very sick children, those with medial conditions such as diabetes and also people with defective immunity these are people with diseases that compromise their immune system or people who are being treated with chemotherapy or steroids.
Controlling Nosocomial infections include:
1. Hand hygiene this is one of the simplest approach to preventing the spread of infections. Surgical team personnel should wash their arms and forearms before a procedure and put on sterile gloves.
2. Environmental hygiene one if the most common sources of transmission of infections is environmental surfaces. Certain types of microbial bacteria are capable of surviving on environmental surfaces for months at a time. When healthcare providers or patients touch these surfaces with their skin the bacteria can be transmitted, causing infection. Thus is it essential that the environment be kept clean and disinfected.
3. Screening and cohorting patients: Screening can help identify what patient has what infection and can immediately be treated, also it is essential that patients who are suffering from the same disease or infection should be kept together in a designated area to avoid it from spreading to patients who don’t have it.
4. Vaccinations, organisations must make sure that recommended vaccinations are being administered to their staff so that they don’t pass on a infections to the patients.
5. Surveillance, organisations should gather data regarding infection patterns at their facility. They should also regular assess current infection prevention protocols. Having a robust infection surveillance program helps organization measure outcomes, assess processes of care and promote patient safety.
6. Antibiotic stewardship, the misuse and overuse of antibiotics can put patients at a risk of contracting infections, Inappropriate antibiotic use may also result in patients becoming resistant to some drugs. If those patients contract an infection, it becomes harder to treat them and the risk of it spreading increases.
7. Care coordination, Breakdown of communication in the surgical preparation, planning and postoperative care management among various care providers during the care transition process can lead to surgical site infections that could otherwise be avoided, there needs to be coordination of care and communication within the surgical team as well. There is a risk of breaking the sterile field in the surgery room particularly around the portion of the surgical procedure when multiple, critical activities are taking place at the same time that require staff to multitask, she says. Care coordination goes a long way in preventing surgical site infections.
8. Following the evidence, keeping alongside of the latest findings regarding the spread of infections and strategies for prevention is essential for a successful infection prevention program. However, it is also important to first look at the reality of your organization’s processes and perform your own gap assessment before adopting new practices. What is new in the infection prevention field may not necessarily be the best fit for the organization.
Vaccination has made an enormous contribution to global health. Two major infections, smallpox and rinderpest, have been eradicated. Despite these successes, approximately 6.6 million children still die each year and about a half of these deaths are caused by infections, including pneumonia and diarrhoea, which could be prevented by vaccination. Enhanced deployment of recently developed pneumococcal conjugate and rotavirus vaccines should, therefore, result in a further decline in childhood mortality. Development of vaccines against more complex infections, such as malaria, tuberculosis and HIV, has been challenging and achievements so far have been modest. Final success against these infections may require combination vaccinations, each component stimulating a different arm of the immune system. In the longer term, vaccines are likely to be used to prevent or modulate the course of some non-infectious diseases. Progress has already been made with therapeutic cancer vaccines and future potential targets include addiction, diabetes, hypertension and Alzheimer’s disease.
A vaccine is a biological preparation that provides active acquired immunity to a particular disease. A vaccine typically contains an agent that resembles a disease-causing microorganism and is often made from weakened or killed forms of the microbe, its toxins or one of its surface proteins. The agent stimulates the body’s immune system to recognize the agent as a threat, destroy it, and keep a record of it so that the immune system can more easily recognize and destroy any of these microorganisms that it later encounters.
Cholera vaccines can be oral or injectable. The oral vaccines are generally of two forms, inactivated and attenuated. Two variants of the inactivated oral vaccine currently are in use: WC-rBS and BivWC. WC-rBS is a monovalent inactivated vaccine containing killed whole cells of V.cholerae O1, plus additional recombinant cholera toxin B subunit. BivWC is a bivalent inactivated vaccine containing killed whole cells of V.cholerae O1 and V. The vaccine acts by inducing antibodies against both the bacterial components and the cholera toxin which is a protein complex secreted by the bacterium Vibrio cholera. The antibacterial intestinal antibodies prevent the bacteria from attaching to the intestinal wall, thereby impeding colonisation of V. cholerae O1. The anti-toxin intestinal antibodies prevent the cholera toxin from binding to the intestinal mucosal surface, thereby preventing the toxin-mediated diarrhoeal symptoms. he injected cholera vaccines are effective for people living where cholera is common. They offer some degree of protection for up to two years after a single shot, and for three to four years with annual booster. They reduce the risk of death from cholera by 50% in the first year after vaccination.
Anthrax disease can occur in people who are exposed to an infected animal or other source of anthrax bacteria. Anthrax disease can occur in people who are exposed to an infected animal or other source of anthrax bacteria. Anthrax is spread to a human through the skin, the stomach, or the lungs. The bacteria can enter the skin through a cut or wound that comes into contact with products from an infected animal such as meat. Anthrax Vaccine Adsorbed is a vaccine which treats anthrax. The vaccine works by inducing antibodies raised against PA that may contribute to protection by neutralizing the activities of the cytotoxic lethal toxin and edema toxin of anthrax. Anthrax vaccine does not contain live or killed forms of the bacteria that causes anthrax.
Infections can manifest themselves through intracellular and extracellular bacteria.
Extracellular bacteria do not invade cells. Instead they proliferate in the extracellular environment which is enriched with body fluids. For example, P. aeruginosa is a non-invasive extracellular infection, that rapidly spreads to various tissues extracellular bacteria do not have the capacity to survive the intracellular environment or to induce their own uptake by most host cells. Intracellular bacteria invade host cells when it gives them selective advantage. Bacteria that can enter, survive and proliferate within eukaryotic cells are shielded from humoral antibodies and can be eliminated only by a cellular immune response. However, these bacteria must possess specialized mechanisms to protect them from the harsh environment of the lysosomal enzymes encountered within the cells. An example of this are small colony variants (SCVs) of S. aureus.
Extracellular infection
P. aeruginosa has several important virulence factors that serve different purposes. Including adhesion, siderophores, elastase, exo-toxins, and coordinating. The interaction between P. aeruginosa type IV pili and the Asialo-GM1 mediates bacterial adherence to the epithelial cells. Typically, many pathogens have a mechanism to steal iron from the host cell, as iron is often a limiting nutrient. For pseudomonas, the main molecule for transport is the peptide pyoverdin which is an ion chelator. It is excreted into the medium in its iron free form. The iron-bound form is recognised by ferric-pyoverdin recognition (Fpv) receptors (FpvA/FpvB) which release and internalise the iron from pyoverdine in a TonB-dependent mechanism. Elastase is a major virulence factor in P. aeruginosa , as it is believed it causes extensive tissue damage during infection in the human host. Elastase cleaves the connective tissue, IgA and IgG. Other immune-regulatory factors include the loss of flagellar synthesis, as the flagellin which makes up the flagella is an immunostimulant. P. aeruginosa has several independently regulated systems that produce toxins, including type-3-secretion system (T3SS), pyocyanin and cyanide synthesis. The T3SS acts like a molecular needle that injects toxins into the cytoplasm of the target organism. Most T3SS exo-toxins affect eukaryotic signalling pathways and thus interfere with a range of function in target cell physiology, e.g. arranging and maintaining the cytoskeleton. Pyocyanin disturbs the redox balance. P. aeruginosa can produce cyanide, which disrupts ATP generation via oxidative phosphorylation by blocking complex IV. In Pseudomonas, production of pyocyanin and proteases like elastase in quorum sensing (QS)-controlled, pyoverdin and cyanide is part-controlled, as is the T3SS. Different QS systems exist and have complex interactions.
Intracellular infection
SVCs They are auxotrophic for menadione, haemin or thymidine and have phenotypic traits making them well adapted for intercellular survival. S. aureus express microbial surface components recognising adhesive matrix molecules (MSCRAMMs) to adhere to host cells. MSCRAMMs are used to bind directly to the host cell surface membrane or to ligands such as fibronectin. Uptake is the attachment to the host cell which causes changes in the host cell cytoskeleton leading to forced phagocytosis in non-professional phagocytes. An interaction with integrin is the start point for S. aureus entering epithelial cells. Due to integrin-mediated signal transduction, integrin-linked kinase (ILK) activates leading to the reorganization of the actin cytoskeleton. S. aureus needs ILK activation to infiltrate epithelial cells. SCVs invade non-professional phagocytes more because of an increased expression of MSCRAMMs. SCVs cause host cell damage as they decreased production of alpha hemolysin and toxic shock syndrome toxin 1 (TSST-1). Alpha hemolysin is a pore forming toxin transcribed by the hla gene that can lead to the lysis of cells. TSST-1 is a toxin that activates the immune system leading to host immune cell-mediated cytotoxicity. Decreased production of such toxins allows the infected cell to survive for longer to accommodate the bacteria. SVCs have shown immune system resistance as they can resist lysosome bactericides better than normal colony variants. They also have reduced membrane potential that protects them from cationic proteins. SCVs also have increased polysaccharide intercellular adhesin which allows resistance to neutrophil’s non-oxidative defense mechanisms. Therefore, SCVs resist cytoplasmic defensive allowing them to survive for extended periods of time. Intracellular infections proliferate in the cells they invade as opposed to outside the cell. SCVs noticeably proliferate more than normal phenotype colonies.
Cannabinoids are a diverse class of chemical compounds that occur naturally in the human body (endocannabinoids) and cannabis plants (phytocannabinoids). Interactions with the endocannabinoid system (ECS) trigger the release of neurotransmitters triggering various physiological changes.
There are up to 113 different types of Cannabinoids such as CBG, CBC, CBD, THC, CBN and CBDL, all of which are used for different therapeutic or recreational reasons due to their difference in chemical structures and receptors where they bind.
For instance, CBD, CBG and CBC are non-psychoactive agents yet THC, CBN and CBDL are known for their psychoactive properties and bind mainly to CB1. There are three main subgroups: endocannabinoids, phytocannabinoids and artificially made synthetics.
Phytocannabinoids include Cannabidiol (CBD), one of the most abundant types of Cannabinoids found in and extracted from industrial hemp. It has anti-inflammatory, antioxidant, analgesic and anti psychotic properties thus is used to treat vomiting and nausea, epilepsy, oxidative injury and anxiety. Tetra-hydrocannabinol (THC), on the other hand is the рrіmаrу psychoactive Cаnnаbіnоіd found in cannabis is used for palliating neuropathic pain, overactive bladder and spasticity. THC has a strong affinity to and activates CB1 whereas CBD does not. CBD can counteract the psychoactivity of THC due to its relations to CB1 and CB2. The receptors CB1 and CB2, both coupled with g-proteins, have a significant role in the mechanism of Cannabinoids. CB1 is located in the brain region and CNS, where it impacts the limbic system by converting signals as an outcome to CNS-active components of Cannabis. CB2 is primarily expressed in the immune system and peripheral nerve terminals, playing a role in antinociception. Endocannabinoids are naturally manufactured endogenous ligands in the body and include 2-arachidonoylglycerol and palmitoylethanolamide. Some are released from depolarised neurons and bind to CB1 receptors in the pre-synaptic neuron. This will cause a reduction in the release of GABA or glutamate, leading to short-term plasticity. Therefore, the CB1 receptor is the psychoactive cannabinoid receptor. Contrarily, CB2 does not have a psychoactive effect as it is mainly located in peripheral organs thus is able to influence fundamental body functions.
Marinol is a synthetic and pharmaceutical stereo isomer of THC(delta-9-tetrahydrocannabinol)and used as an appetite stimulant for treating individuals with HIV/AIDS and a form of treatment for chemotherapy-induced nausea and vomiting.
ØRoutes of Administration:
Marinol is administrated through oral capsules containing 2.5 mg, 5 mg, or 10 mg of dronabinol. This is a convenient route and allows for an enhanced effect of non-absorbed drugs on the GI tract.
ØPharmacokinetics Absorption: Around 90%–95% of Marinol is absorbed after a single dosage capsule. However, as a consequence of first pass high lipid solubility and hepatic metabolism, 10%–20% of the administrated dose is able to get to the systemic circulation. Distribution:
The distribution of Marinol is the movement of drug between blood and extra vascular tissues. The plasma protein binding of dronabinol is approximately 97% and around 10L/kg of Marinol is distributed due to the substances lipid solubility. Metabolism: Marinol is metabolized to 11-OH-delta-9-THC as it goes through a considerable first-pass hepatic metabolism via Microsomal hydroxylation. Cytochrome p450, enzymes CYP2C9 and CYP2C19 allow for this action to occur producing both active and inactive metabolites. The concentration of these metabolites is highest at around 0.5 to 4 hours after oral consumption. Excretion:
Over 55% of the Marinol along with its bio transformation by-products are excreted in faeces and around 10%-15% is detected from urine after 72 hours. Furthermore, less that 5% is recovered in the faeces unchanged. After 5 weeks and a single dose of the Marinol, low levels of metabolites are still found in the urine and faeces. The primary metabolite found in urine is ester glucuronic acid and THC-COOH whereas in the faeces mainly 11-OH-THC is found.
ØPharmacodynamics Mechanism of action:
Marinol has a complex effect on the CNS and its central sympathomimetic activity. They are stereo isomers of THC thus have partially agonist properties at CB1 and CB2. Their psychoactive effects are mainly mediated by the activation of CB1. This decreases the concentration of cAMP signal transaction is exerted by Cannabinoid receptors, leading to a decreased neuron excitability. Marinol inhibits vomiting by effecting the control mechanism in the medulla oblongata. They are able to generate antiemetic effects by either altering the upper cortex, which in turn influences the medulla or mediating Cannabinoid receptors in the ASNTS, a region directly connected to the hypothalamus. They are also able to influence antiemetic effects by acting to oppose the effects of serotonin (5-HT3). This will inhibit the release of neurotransmitters from vagal afferent terminals that induce vomit.The CB1 receptors in the lateral hypothalamus will also affect the appetite stimulating properties of this drug. Furthermore, it can also be mediated by ASNTS. -Marinol shows a reversible effect on appetite, cognition, mood and perception. This is related to the dosage, where there is a positive correlation between an increasing frequency and dosage.
-It has an onset of action of 0.5 to 1 hours and peak effect at 2 to 4 hours. The psychoactive results last 4 to 6 hours. Furthermore, its appetite stimulant effects last for over 24 hours after a single dose usage.
-A rapidly diminishing response and tolerance for Marinol can be developed suggesting there is an impact on sympathetic neurons. However, they don’t occur to the appetite stimulant effects. -Tachycardia and conjunctival injections can occur due to dronabinol-induced sympathomimetic activity where orthostatic hypotension is experienced. There is an inconsistent effect on blood pressure.
Therapeutic effects:
Marinol is a pharmaceutical product used for several therapeutic reasons. It can be used as an appetite stimulant used for patients dealing with anorexia or severe weight loss during HIV/AIDS. It is also used to treat individuals for nausea and vomiting caused by chemotherapy. This is only taken when previous medical attempts in palliating these symptoms were not successful. Furthermore, Marinol has also been found to reduce cannabis withdrawal symptoms.
Side effects:
There are many side effects to using Marinol. These can vary from common to serious and abnormal.
Common side effects will include:
Mood changes
Dizziness
Anxiety
Headaches
Stomach/ Abdominal pain
Lack of coordination
Vomiting
Fatigue
Insomnia
However, more severe side effects can occur when using Marinol including:
Rapid heart rate
Fainting
Seizures
Hallucinations
This will require immediate attention from a medical expert.
Marinols synthetically formed properties show a unique mechanism of action that specifically minister to appetite stimulation and antiemetic properties. A large percentage of this drug is absorbed, yet an insignificant amount is able to enter the systemic circulation. This means the dosage given is crucial as first pass effects must be considered. Marinols are effective last resort drugs as they do contain a wide range of side effects and thus must be handled with precaution.
To survive in the presence of an antibiotic, bacterial organisms must be able to disrupt one or more of the essential steps required for the effective action of the antimicrobial agent.
The intended modes of action of antibiotics may be counter-acted by bacterial organisms via several different means. This may involve preventing antibiotic access into the bacterial cell or perhaps removal or even degradation of the active component of the antimicrobial agent. No single mechanism of resistance is considered responsible for the observed resistance in a bacterial organism. In fact, several different mechanisms may work together to confer resistance to a single antimicrobial agent.
– By preventing of the antimicrobial form reaching its target by reducing its ability to penetrate into the cell, Antimicrobial compounds almost always require access into the bacterial cell to reach their target site where they can interfere with the normal function of the bacterial organism. Porin channels are the passageways by which these antibiotics would normally cross the bacterial outer membrane. Some bacteria protect themselves by prohibiting these antimicrobial compounds from entering past their cell walls. For example, a variety of Gram-negative bacteria reduce the uptake of certain antibiotics, such as aminoglycosides and beta lactams, by modifying the cell membrane porin channel frequency, size, and selectivity. Prohibiting entry in this manner will prevent these antimicrobials from reaching their intended targets that, for aminoglycosides and beta lactams, are the ribosomes and the penicillin-binding proteins (PBPs), respectively.
– By expulsive of antimicrobial agents from the cell via general or specific efflux pumps, to be effective, antimicrobial agents must also be present at a sufficiently high concentration within the bacterial cell. Some bacteria possess membrane proteins that act as an export or efflux pump for certain antimicrobials, extruding the antibiotic out of the cell as fast as it can enter. This results in low intracellular concentrations that are insufficient to elicit an effect. Some efflux pumps selectively extrude specific antibiotics such as macrolides, lincosamides, streptogramins and tetracyclines, whereas others (referred to as multiple drug resistance pumps) expel a variety of structurally diverse anti-infectives with different modes of action.
– By inactivation of antimicrobial agents via modification or degradation, Another means by which bacteria preserve themselves is by destroying the active component of the antimicrobial agent. A classic example is the hydrolytic deactivation of the beta-lactam ring in penicillins and cephalosporins by the bacterial enzyme called beta lactamase. The inactivated penicilloic acid will then be ineffective in binding to PBPs (penicllin binding proteins), thereby protecting the process of cell wall synthesis.
– By medication of the antimicrobial target within the bacteria, Some resistant bacteria evade antimicrobials by reprogramming or camouflaging critical target sites to avoid recognition. Therefore, in spite of the presence of an intact and active antimicrobial compound, no subsequent binding or inhibition will take place.
Beta-lactam antibiotics share the structural feature of a beta-lactam ring. This feature is responsible for inhibition of bacterial cell wall synthesis. The target molecules are peptidoglycan cross-linking enzymes (e.g. transpeptidases and carboxypeptidases) which can bind beta-lactam antibiotics (penicillin binding proteins, PBP). Bacterial cell death is initiated by beta-lactam antibiotic-triggered release of autolytic enzymes.